
BIG PHARMA +
BIG MEDICAL +
BIG GOVT =
CRIMINAL CONSPIRACY
TO FALSELY CONVICT AND
MURDER INNOCENT PARENTS TO
COVER-UP VACCINE-INDUCED DEATHS
SOTN Editor’s Note:
“However, there is one piece to this case that was left out. She was arrested a year later, but after she became the plaintiff in a racketeering case against the AAP. Since she was arrested, the AAP asked for the case to be dismissed. Unless we call out and recognize this is how they operate, it will be business as usual.”
— Comment post by CHop
What makes the following egregious abuse by the U.S. Criminal Justice System particularly malicious and malevolent can be understood by the preceding comment which was posted under the article below.
State of the Nation
July 18, 2026
The Shaw Twins Case: A Mother, a Murder Charge, and Eighty Years of Evidence No One Wants to See
Sayer Ji

How five vaccines and a bottle of Tylenol converge on the infant brainstem — and why the medical examiner’s “smothering” verdict is the last stage of a century-long classification laundry
On the night of April 30, 2025, Andrea Shaw put her 18-month-old twins to bed in a small house in Payette, Idaho. She had watched them collapse eight days earlier — blue-lipped, eyes rolled back, unable to walk — hours after their pediatrician injected them with five vaccines during a single well-baby visit. The emergency room that night wrote “post-immunization reaction” in the chart, handed her a bottle of children’s Tylenol, and sent her home. For seven more days the twins were listless, feverish, refusing food, passing green diarrhea. On the morning of May 1, she found Dallas and Tyson cold and still in their shared crib.

In July 2026, prosecutors indicted her for their murder — alleging she smothered both children in a single night. She is being held without bail and faces the death penalty.[^1] What the state of Idaho refuses to see is that the etiology of these deaths is not obscure, not speculative, and not novel. It is, in fact, the most extensively documented — and most systematically suppressed — pediatric toxicology pattern of the past eighty years. Two exposures, biochemically synergistic, converging on the same fragile brainstem structures at precisely the moment when the medical literature predicts fatal apnea. This is not a whodunit. It is a why-won’t-we-look. And it is the inevitable, engineered consequence of a public-health apparatus that has spent forty years insisting — against a mountain of its own peer-reviewed evidence — that all childhood vaccines are “safe and effective” for all children. When the medicine kills, the mother must have.
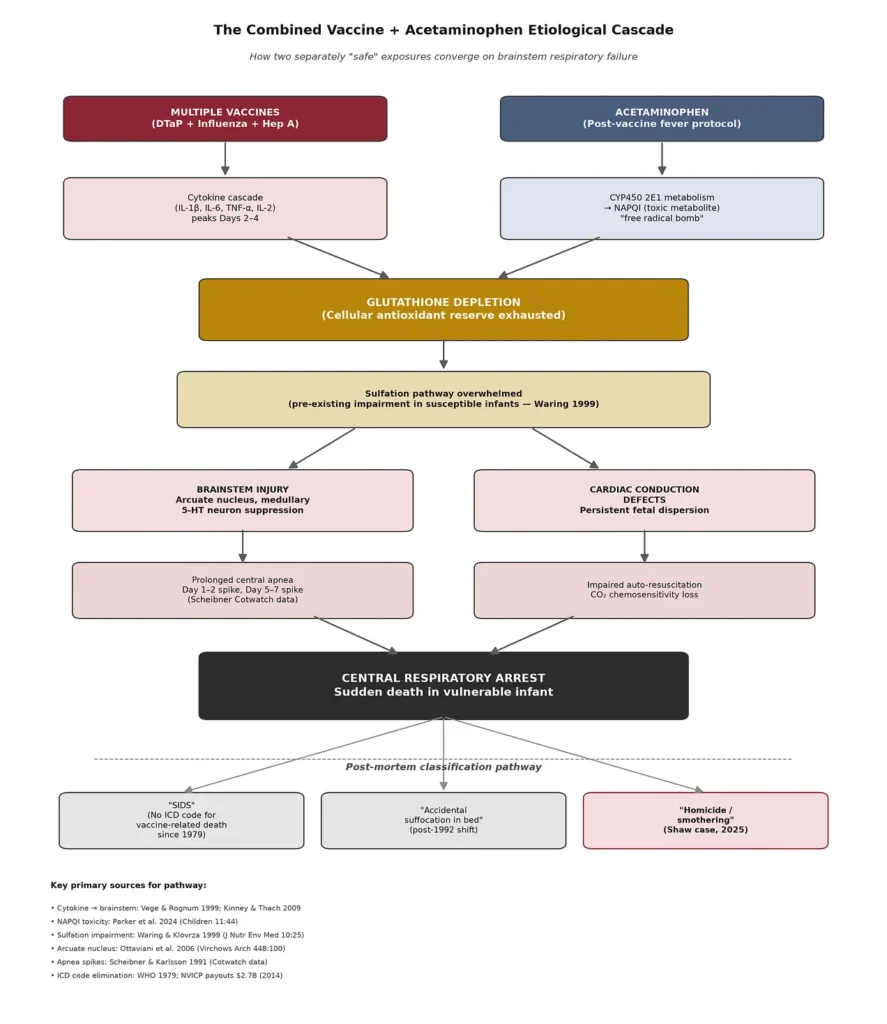
Figure 1. The combined etiological pathway. Two “independently safe” exposures — a multi-antigen vaccine cocktail and acetaminophen given for post-vaccine fever — converge on glutathione depletion, sulfation pathway failure, and brainstem/cardiac injury. The final classification stage on the bottom row shows how the same physiological outcome has been rerouted through three institutional categories over the past four decades.
What the Chart Actually Says
The publicly available record of the Shaw twins’ final week is, on its face, sufficient to raise the diagnostic possibility of vaccine-plus-acetaminophen–induced central apnea in any pediatrician trained before 1986.[2] Consider the timeline:
- April 23, 2025: Dallas and Tyson Shaw, 18-month-old fraternal twins, received five vaccines at a routine well-baby visit — DTaP, influenza (with prior paternal reaction history), and hepatitis A.[1] Both Andrea Shaw and the twins’ paternal grandmother reportedly warned the pediatrician of the father’s adverse reaction to influenza vaccine. The vaccines were administered anyway.[3]
- April 24: Within twenty-four hours, both twins collapsed. Symptoms included cyanosis (blue lips), rolled-back eyes, inability to walk, and green watery diarrhea. Emergency department documentation records “post-immunization reaction.” The children were sent home with acetaminophen (Tylenol) and popsicles.[1][3]
- April 25 – April 30: Seven days of continued lethargy, severe diarrhea, food refusal, and low-grade illness. Standard pediatric guidance — including the guidance the ER discharge instructions almost certainly reflected — is repeat acetaminophen dosing for post-vaccination symptoms.[4]
- April 30 (evening): The twins were put to bed early.
- May 1 (morning): Both children were found dead, cold, in their shared crib. Autopsy findings included pulmonary vascular congestion.[3]
Dr. Pierre Kory, who reviewed the full medical record, concluded the deaths were consistent with severe apnea induced by the vaccines administered eight days earlier.[2] The state of Idaho, three doctors it declines to identify, and the Payette County prosecutor concluded instead that Andrea Shaw suffocated both of her children in a single night. They cite the pulmonary vascular congestion as consistent with smothering, and note that both twins were found dead simultaneously as evidence against natural causes: “It is also the only reasonable explanation,” prosecutor Michael Duke argued, “for why both would die at the same time, on the same night, in the same room, in the same bed.”[5]
This argument is exactly backwards. The literature on simultaneous twin deaths after vaccination is neither sparse nor recent. It stretches from 1946 to 2025. The Shaw twins are at least the ninth documented pair.
Eighty Years of Simultaneous Twin Deaths After Vaccination
The baseline mathematics is unambiguous. Malloy and Freeman’s 1999 analysis of 172,029 U.S. twin pregnancies over five years identified only seven cases in which both twins died of Sudden Infant Death Syndrome (SIDS), and only one in which both died on the same day — a rate of 0.58 per 100,000 twin pregnancies.[6] The forensic pathologist Millard Bass, cited in the same literature, put the matter plainly: “The likelihood of twin infants dying suddenly and simultaneously of SIDS, a natural disorder, defies credibility.”[7]
And yet the medical literature — peer-reviewed, publicly indexed, largely ignored — contains at least eight sets of twins who died together in tight temporal proximity to vaccination before the Shaw twins made nine. Every one of these cases involved the same pattern: healthy children, routine vaccination, silent death within days:
![YearAgesInterval post-vaccineVaccinesCitation1946Identical twin boys16–20 hoursDiphtheria toxoid + pertussis (2nd dose)Werne & Garrow, JAMA[^8]1985Twin boys2–3 hoursDPTRoberts, Arch Dis Child[^9]1987Twin boys, 5 mo3 hoursDPTCoulter & Fisher[^10]2007Identical twin girls, 15 wk2 daysDPT + Hep B + oral polio (+ acetaminophen for post-vaccine fever)Balci et al., Forensic Sci Int[^11]2010Identical twin boys, 12 wk5 daysDTaP + OPV + Hep B + HibMitchell et al., Int J Legal Med[^12]2013Twin boys, 10 wk10 daysDPT + OPV (1st dose)Huang et al.[^13]2025Boy/girl, 18 mo8 daysDTaP + influenza + hepatitis A (+ acetaminophen at ER Day 1)Shaw twins (case in litigation)[^1]](https://substackcdn.com/image/fetch/$s_!z426!,w_1456,c_limit,f_webp,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fb04f5647-e45b-482a-8aa2-09d0743b3abe_1520x838.png "YearAgesInterval post-vaccineVaccinesCitation1946Identical twin boys16–20 hoursDiphtheria toxoid + pertussis (2nd dose)Werne & Garrow, JAMA[^8]1985Twin boys2–3 hoursDPTRoberts, Arch Dis Child[^9]1987Twin boys, 5 mo3 hoursDPTCoulter & Fisher[^10]2007Identical twin girls, 15 wk2 daysDPT + Hep B + oral polio (+ acetaminophen for post-vaccine fever)Balci et al., Forensic Sci Int[^11]2010Identical twin boys, 12 wk5 daysDTaP + OPV + Hep B + HibMitchell et al., Int J Legal Med[^12]2013Twin boys, 10 wk10 daysDPT + OPV (1st dose)Huang et al.[^13]2025Boy/girl, 18 mo8 daysDTaP + influenza + hepatitis A (+ acetaminophen at ER Day 1)Shaw twins (case in litigation)[^1]")
The 1946 Werne and Garrow case is particularly important because the U.S. Institute of Medicine — an institution not known for its skepticism of vaccination — concluded in its 2003 Immunization Safety Review that “the evidence favors acceptance of a causal relationship between diphtheria toxoid- and whole cell pertussis vaccine and death due to anaphylaxis in infants,” basing this conclusion primarily on the twin case.[14] The IOM has, in other words, already conceded the mechanism at the level of individual case reports. What it has never accepted is the population-level extrapolation.
The 2007 Balci case is even more directly relevant to the Shaw twins. Fifteen-week-old identical girls in Istanbul received a second dose of DPT, first dose of hepatitis B, and second dose of oral polio. They developed fever on Day 1. Their mother administered acetaminophen per pediatric guidance. Two days later, both were dead in their crib, supine, no signs of struggle.[11] The Turkish Institute of Forensic Medicine ruled the deaths “consistent with SIDS.” The parallel to Payette is exact: vaccines + post-vaccine acetaminophen + simultaneous death of twins within days.
The Cytokine Storm and the Vulnerable Brainstem
The mechanistic evidence for vaccine involvement in infant death does not depend on twin cases. It has been reconstructed in molecular detail from three converging bodies of evidence: cytokine physiology, brainstem neuropathology, and cardiac conduction pathology.
The cytokine cascade. Foreign antigens introduced via vaccination activate the innate immune system within hours, producing interleukin-1β, interleukin-6, tumor necrosis factor-α, and interleukin-2. In infants, these cytokines cross the immature blood-brain barrier and act directly on the medullary serotonergic (5-HT) neurons that regulate respiratory chemosensitivity and auto-resuscitation from apnea. Kinney and Thach’s 2009 New England Journal of Medicine review of the neuropathology of SIDS documents that impaired 5-HT signaling in the medulla is the single most consistent postmortem finding across SIDS cohorts.[^15] Vege and Rognum showed as early as 1999 that SIDS infants exhibit elevated IL-6 in cerebrospinal fluid, with the identical topographic distribution — solitary nucleus tractus, spinal trigeminal nucleus, arcuate nucleus — in both SIDS cases and non-SIDS infants dying of acute infectious illness.[16] The physiological effect: prolonged central apnea, inhibited arousal from hypoxia, failure to auto-resuscitate.
The brainstem lesion. Ottaviani, Lavezzi, and Matturri, working at the University of Milan, published in Virchows Archiv in 2006 a detailed neuropathological analysis of a three-month-old female infant who died within hours of hexavalent vaccination. Serial-section examination of the brainstem revealed bilateral hypoplasia of the arcuate nucleus. The cardiac conduction system showed persistent fetal dispersion and resorptive degeneration. The authors concluded that the case “offers a unique insight into the possible role of hexavalent vaccine in triggering a lethal outcome in a vulnerable baby.”[17] They subsequently expanded their series to 110 SIDS cases, finding that 13 (11.8%) had died within 1–7 days of hexavalent vaccination, and in one case identified acute encephalitis of the tractus solitarii nucleus in the brainstem — a finding, they noted, that cannot be explained by developmental abnormality alone.[18] Zinka et al. in Munich independently reported six additional cases of unexplained sudden infant death within 48 hours of hexavalent vaccination the same year.[19]
The regulatory signal. Von Kries et al., analyzing German pharmacovigilance data, found that in the second year of life — precisely the Shaw twins’ age range — the standardized mortality ratio for sudden unexpected death within one day of hexavalent vaccination reached 31.3 (95% CI 3.8–113.1) and within two days 23.5 (95% CI 4.8–68.6). The authors, writing in the European Journal of Pediatrics, described these findings as “a signal for one of the two hexavalent vaccines which should prompt intensified surveillance.”[20] The European Medicines Agency’s response was to withdraw one of the two hexavalent formulations (Hexavac) from the market — while simultaneously insisting there was no evidence of a causal relationship. The Italian PLoS One case series subsequently found a 2.0-fold risk ratio (95% CI 1.2–3.5) for sudden unexpected death in the seven days following first-dose hexavalent vaccination.[21] Kuhnert et al. reported a 16-fold risk elevation following the fourth dose of penta/hexavalent vaccine.[22]
The population signal. Goldman and Miller’s 2011 analysis of 34 developed nations found a Pearson correlation of r = 0.992 (p = 0.0009) between the number of scheduled infant vaccine doses and the infant mortality rate.[23] Nations requiring more doses have higher infant mortality. Their 2012 VAERS analysis showed that infants receiving five to eight vaccines simultaneously — precisely the Shaw twins’ exposure — had a hospitalization rate ratio of 1.5 (95% CI 1.4–1.7) and a mortality rate 50% higher than infants receiving fewer.[24] Hooker and Miller’s 2021 Toxicology Reports analysis of 2,605 VAERS infant death reports over three decades found that 58% occurred within three days of vaccination and 78% within one week — a temporal clustering the authors described as “highly suggestive of a causal relationship.”[25]
The picture that emerges is not ambiguous. It is a coherent, cross-decade, cross-methodology body of work spanning pathology, epidemiology, VAERS analysis, ecological correlation, and pharmacovigilance signal detection.
The Second Poisoning: Acetaminophen as Etiological Amplifier

Here is where the Shaw twins case departs from any prior public discussion of their deaths — and where the mechanistic evidence becomes most damning.
Acetaminophen (paracetamol; Tylenol) is not a neutral fever reducer. It is a xenobiotic that, in infants, is preferentially metabolized through cytochrome P450 2E1 into N-acetyl-p-benzoquinone imine (NAPQI) — a reactive metabolite that immunologist William Parker, formerly of Duke University and author of nearly 200 peer-reviewed papers, has described as a “free radical bomb.”[26] NAPQI’s primary detoxification pathway requires glutathione, the cell’s central antioxidant reserve. When glutathione is intact, NAPQI is neutralized. When glutathione is depleted, NAPQI attacks membrane lipids, mitochondrial proteins, and — critically for the Shaw twins — the same brainstem structures already sensitized by vaccine-induced cytokines.
For a far deeper dive, I’ve written extensively on the topic of Tylenol’s wide-ranging and underreported toxicity in my Tylenol Investigation series here on Substack.
The infant biochemical vulnerability is well-established:
- Immature glucuronidation. Newborns and toddlers clear acetaminophen inefficiently through the mature glucuronidation pathway, shunting a higher proportion into the NAPQI-producing CYP450 2E1 pathway. The metabolic profile in early infancy resembles that of cats — an animal famously fatal-to-Tylenol.[26]
- Impaired sulfation. Waring and Klovrza documented in 1999 that children with autism — and, by extension, an unknown fraction of neurotypical children with subclinical sulfation deficits — exhibit impaired sulfation, a critical secondary detoxification pathway for acetaminophen.[27] The Shaw twins’ baseline sulfation capacity was never measured. It never is.
- Glutathione baseline in acute illness. Infants who are already ill, febrile, inflamed, or under oxidative stress — for instance, infants in the immediate post-vaccination cytokine surge window — have depleted glutathione reserves before the first dose of acetaminophen enters the system.[26][28]
The Schultz et al. 2008 study in Autism is the single most important epidemiological finding for understanding the Shaw case, and it has been almost totally ignored in mainstream medical discourse. Using a parent-survey design covering post-MMR vaccination exposures, Schultz’s team found that children given acetaminophen after MMR had approximately 8-fold higher odds of developing autism (OR ~8.2) compared to children given ibuprofen or no analgesic. Children given ibuprofen showed no elevated risk. Among children who experienced post-vaccination fever specifically, the acetaminophen-associated regressive autism incidence was twenty-fold higher.[29] The vaccine alone did not produce the effect. The vaccine plus acetaminophen did.
The Boston Birth Cohort — an NIH-funded prospective study measuring acetaminophen biomarkers directly in umbilical cord blood — found that infants in the highest cord-blood acetaminophen quartile had 3.6 times the risk of subsequent autism diagnosis compared to those in the lowest, with clear dose-response.[30] The 2021 international consensus statement in Nature Reviews Endocrinology, co-authored by 91 scientists, formally called for precautionary restriction of acetaminophen use during pregnancy on the basis of accumulating neurodevelopmental evidence.[31]
The convergence with vaccination is not coincidental. Standard American pediatric practice, throughout the 1980s and 1990s and continuing into the present, has been to preemptively or reactively administer acetaminophen for post-vaccination fever.[^4] The result is that virtually every American child born in the past four decades has been exposed to combined vaccine + acetaminophen at the exact developmental windows — 2, 4, 6, 12, 15, and 18 months — when the medullary serotonergic system is most vulnerable. The Shaw twins were poisoned twice: once by five simultaneous vaccine antigens depleting their glutathione reserves and priming their brainstems for apnea, and again by the acetaminophen given by an emergency department to manage the recognized “post-immunization reaction” — the very drug most likely to finish what the vaccines started.
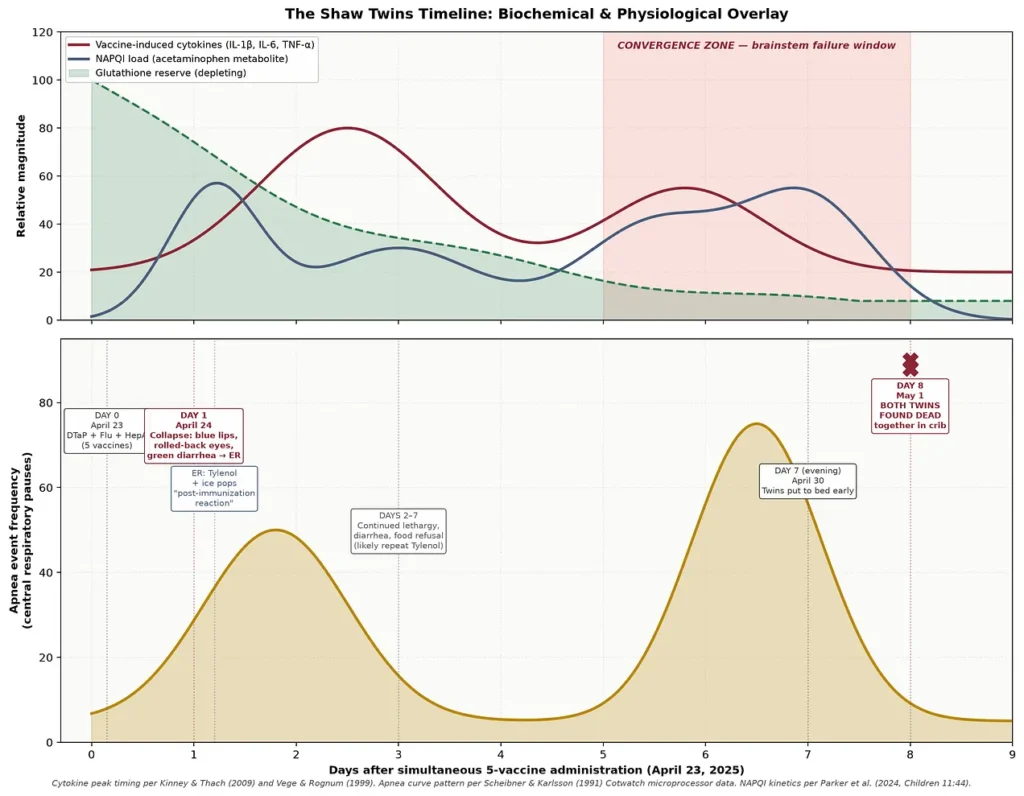
Figure 2. Biochemical and physiological overlay of the Shaw twins’ final eight days. The upper panel plots relative magnitude of vaccine-induced cytokines, acetaminophen-derived NAPQI, and depleting glutathione reserve. The lower panel shows the two well-documented apnea event peaks — one Day 1–2 (per Scheibner’s 1991 Cotwatch data) and a second, larger peak Day 5–7 — against the clinical timeline. All three biochemical curves converge fatally in the Day 5–8 window when both twins died.
The Angela Cannings Precedent — When “Statistical Impossibility” Convicts the Innocent

The prosecution’s central theory in the Shaw case — voiced by Payette County prosecutor Michael Duke as “the only reasonable explanation for why both would die at the same time, on the same night, in the same room, in the same bed”[5] — is not a novel argument. It is a nearly verbatim recapitulation of the theory that sent Angela Cannings, Sally Clark, and Donna Anthony to prison in Britain in the late 1990s and early 2000s, and that the England and Wales Court of Appeal ultimately declared unsafe as a matter of law.[40a]
Angela Cannings lost three infants — Gemma (13 weeks, 1989), Jason (7 weeks, 1991), and Matthew (18 weeks, 1999). Doctors initially diagnosed the first as SIDS. When the second and third died, prosecutors argued that multiple unexplained infant deaths in a single family were so statistically improbable that homicide was the more likely explanation. Their star witness was pediatrician Sir Roy Meadow, then president of the British Paediatric Association, whose “Meadow’s Law” declared: one infant death is a tragedy, two is suspicious, three is murder unless proven otherwise. In 2002 Cannings was convicted of murdering Jason and Matthew and sentenced to life in prison. There was no confession, no eyewitnesses, no physical evidence of smothering, no injuries — only the statistical argument.[^40a]
On December 10, 2003, after Cannings had served twenty months, the Court of Appeal overturned her convictions. The court’s holding is directly applicable to the Shaw prosecution: where a case depends “exclusively, or almost exclusively, on a serious disagreement between distinguished and reputable experts,” it is “unwise, and therefore, unsafe” to permit a conviction to stand.[^40a] Within weeks, Attorney General Lord Goldsmith announced a systematic review of hundreds of similar cases. Sally Clark’s conviction was overturned the same year. Donna Anthony was freed in 2005. In every one of those cases, subsequent scientific investigation revealed genetic, metabolic, or environmental causes for infant deaths that had been declared “statistically impossible” and therefore homicidal.[40a]
The parallels to the Shaw case are exact:
- Statistical-impossibility theory of guilt. Duke’s “only reasonable explanation” argument is Meadow’s Law transposed to Idaho. Both rest on the premise that unusual clusters of infant death in one family cannot be natural. Both ignore that vaccine-associated twin death is a documented, recurring pattern in the peer-reviewed literature since 1946.
- No physical evidence of homicide. As in Cannings, there is no confession, no eyewitness, no injury, no forensic marker consistent with smothering — only pulmonary vascular congestion, a finding equally consistent with the vaccine-plus-acetaminophen etiology described above.
- Reliance on disputed expert opinion. Idaho prosecutors cite three unnamed physicians who “ruled out vaccines” without producing their credentials, methodology, or reports. Dr. Pierre Kory, who has reviewed the full medical record, has publicly stated the deaths are consistent with vaccine-induced apnea.[^2] This is precisely the “serious disagreement between distinguished and reputable experts” that the Cannings court held renders prosecution unsafe.
- Genetic/metabolic susceptibility ignored. In the post-Cannings British reviews, cases repeatedly turned on inherited disorders — Long QT syndrome, medium-chain acyl-CoA dehydrogenase deficiency, and other channelopathies that produce apparent “SIDS” clusters in siblings. The Shaw twins’ documented paternal history of adverse vaccine reaction points to precisely such a susceptibility, and Ottaviani’s neuropathological literature identifies at least a dozen predisposing factors that would explain simultaneous death after simultaneous exposure.[17][25]
As attorney Chad Davenport told The Defender in July 2026: “The Angela Cannings case taught us a hard lesson: Even top medical experts can be wrong, and guesswork should never replace hard evidence. When dealing with sudden, unexplained tragedies like the Andrea Shaw case, the justice system cannot afford to rush to judgment. If police and medical examiners ignore a family’s medical history or dismiss other possible causes right out of the gate, we risk putting another innocent mother behind bars.”[40a]
The Cannings precedent is not binding on an Idaho court. But it is directly persuasive authority on the fundamental due-process question at the heart of the Shaw case: whether a prosecution may proceed to conviction on nothing more than the statistical improbability of a natural explanation, when a documented natural explanation exists in the peer-reviewed literature and reputable experts disagree with the state’s theory. Under the Cannings standard, this prosecution should not go forward.
The Classification Laundry
If the etiology is so well-established, why is Andrea Shaw in a jail cell? Why did three unnamed physicians “rule out” vaccines as a cause of death? Why did the Payette County coroner refuse to release the autopsy? The answer requires understanding the institutional architecture that has, over the past half-century, systematically absorbed vaccine-related infant deaths into administrative categories that make them statistically invisible.
The mechanism operates in three layers:
Layer 1 — Eliminated ICD codes. The International Classification of Diseases contains 130 official categories for infant cause of death. Prior to 1979, one of those categories was “death from prophylactic vaccination.” That code was eliminated. There is now no ICD code under which a medical examiner can classify a vaccine-attributable infant death.[32] The category was replaced, functionally, by the diagnosis of exclusion known as SIDS — a category that did not exist before 1973, invented in that year to accommodate an epidemic of unexplained infant deaths that had emerged in the 1960s alongside the mass rollout of DPT, oral polio, and measles vaccines.[32]
Layer 2 — Reclassification. After the 1992 American Academy of Pediatrics “Back to Sleep” campaign was credited with an 8.6% annual decline in SIDS between 1992 and 2001, Malloy and MacDorman’s Pediatrics analysis demonstrated that deaths coded as “accidental suffocation in bed” had risen 11.2% annually over the same period. The reclassification accounted for approximately 90% of the apparent SIDS decline.[33] The deaths did not decrease. Their names did.
Layer 3 — Prosecutorial classification. The Shaw case represents the newest layer of this laundry: when the vaccine + acetaminophen exposure produces simultaneous twin death — a pattern that cannot plausibly be classified as SIDS given the extreme statistical improbability — the deaths are reassigned to homicide. The mother is prosecuted. The vaccines and the acetaminophen never appear in the courtroom except as items her defense attorney must struggle to introduce over prosecutorial objection. The National Vaccine Injury Compensation Program has paid out over $5.4 billion in compensation for vaccine injuries and deaths since 1988,[34] many of the settled infant-death cases having originally carried a SIDS or suffocation diagnosis. This is public knowledge. It plays no role in Idaho’s case against Andrea Shaw.
The institutional pattern is not accidental. It is the same governance-by-classification that has characterized every major pharmaceutical harm suppression of the past century — from thalidomide to Vioxx to opioids. The specific stakeholders in the vaccine + acetaminophen dyad are not obscure: Johnson & Johnson has been simultaneously one of the largest global manufacturers of both pediatric vaccines and Tylenol (until the 2023 spinoff of Kenvue), and William Parker’s Duke University laboratory was shuttered in 2021 — with the department deeming further acetaminophen-autism research “not in the strategic best interest” of Duke — while two Duke administrators, including the Chancellor for Health Affairs, simultaneously served on Johnson & Johnson’s Board of Directors.[35] An anonymous donor’s offer to fully fund Parker’s salary and experiments was declined.
Broken Trust: The Tylenol Cover-Up That May Have Damaged Millions of Children
Sayer Ji
Read, share, and comment on the X post dedicated to this thread here: https://x.com/sayerjigmi/status/1966659933694296412
What the Autopsy Should Have Looked For — and Almost Certainly Did Not
The Ottaviani protocol, published in Virchows Archiv in 2006 and refined in the 2014 expanded series, is explicit about what a competent post-mortem examination in a suspected vaccine-associated infant death must include:[17][18]
- Serial sectioning of the brainstem, with specific examination of the arcuate nucleus, the tractus solitarii nucleus, the spinal trigeminal nucleus, and the dorsal vagal nucleus.
- Immunohistochemistry for cytokine expression (IL-1β, IL-2, IL-6, TNF-α) in medullary respiratory control centers.
- Cardiac conduction system examination for persistent fetal dispersion, resorptive degeneration, and sinoatrial/atrioventricular node abnormalities.
- Hepatic and cerebral glutathione measurement, with quantitation of NAPQI-protein adducts as evidence of acetaminophen-induced oxidative stress.
- Beta-tryptase quantitation to evaluate for anaphylactoid mast-cell activation — the mechanism identified in the 2008 Forensic Science International case of an infant dying 24 hours post-hexavalent vaccination.[36]
Payette County coroner Ethan Mittelstadt has stated that the Shaw twins’ autopsy records will remain confidential until the criminal proceedings conclude.[1] There is no public evidence any of the Ottaviani-protocol examinations were performed. The finding of “pulmonary vascular congestion” cited by prosecutors is consistent with mechanical suffocation — but it is equally consistent with central respiratory arrest from any cause, including vaccine + acetaminophen–induced brainstem failure. The prosecutorial argument treats this pathological finding as though it were pathognomonic for smothering. It is not. It is nonspecific. And the standard forensic literature has known this since Werne and Garrow published in 1946.
The Japanese Natural Experiment
The single most persuasive population-level evidence that the vaccine + acetaminophen etiology is not merely temporal correlation comes from Japan. In 1975, following two infant deaths within 24 hours of DPT vaccination, the Japanese government raised the minimum vaccination age from 3 months to 2 years. In the five years preceding the change, Japan had paid 37 compensation claims for infant sudden death within seven days of DPT vaccination. In the 6.5 years following the change, that number dropped to 3.[37] The sudden-death rate per million doses fell from 1.47 to 0.15 — a 90% reduction. Japanese infant mortality overall dropped from 12.4 to 5.0 per 1,000 births over the following decade, moving Japan from an unremarkable position to the lowest infant mortality rate in the world.[^37]
If DPT vaccination in early infancy is causally unrelated to sudden death, this natural experiment should have shown no effect. It showed a 90% effect.
When “Safe and Effective” Becomes a Prison Sentence
The mother of the Shaw twins is in a jail cell today because of a slogan.
“Safe and effective.” “The science is settled.” “Vaccines do not cause SIDS.” “There is no evidence of harm.” These are not scientific statements. They are marketing directives issued by a pharmaceutical-regulatory-media complex that has systematically refused, for more than four decades, to acknowledge what its own peer-reviewed literature — much of it cited in this article — has been documenting since 1946. The refusal is not incidental. It is structural. It is protected by the 1986 National Childhood Vaccine Injury Act, which stripped vaccine manufacturers of liability for pediatric vaccine deaths and injuries and rerouted claims into a no-fault administrative program that has quietly paid out more than $5.4 billion — while the manufacturers whose products caused those injuries assert publicly that no such injuries exist.[34] It is protected by the elimination of the ICD code for vaccine-related death in 1979.[32] It is protected by the SIDS category invented in 1973 to absorb the very deaths this article documents. It is protected by editorial gatekeepers who fast-track rejection of manuscripts challenging the safety consensus,[40] by university administrators who close laboratories rather than publish inconvenient findings,[35] and by media outlets that cover the criminal indictment of Andrea Shaw without mentioning that eight prior sets of twins in the peer-reviewed literature died the same way.
The blanket claim that all childhood vaccines are safe and effective for all children is not merely wrong. It is a category error. No pharmaceutical intervention in the history of medicine has ever been universally safe across all recipients. Aspirin causes Reye’s syndrome. Penicillin causes anaphylaxis. Every drug has a susceptible subpopulation. The peer-reviewed literature identifies at least a dozen susceptibility factors for vaccine-associated infant death: CYP450 polymorphisms, impaired sulfation, arcuate nucleus hypoplasia, MTHFR variants, mitochondrial dysfunction, prior family history of adverse vaccine reaction, prematurity, low birth weight, concurrent illness, multiple simultaneous doses, hot vaccine lots, and post-vaccination acetaminophen exposure.[25][26][28] Every one of these was present or plausibly present in the Shaw twins. The father had a documented prior adverse reaction to influenza vaccine. The mother and grandmother warned the pediatrician. Five vaccines were administered anyway. Acetaminophen was administered on top of them. Both children died.
What follows from a safety claim that admits no subpopulations, no susceptibilities, no bad lots, and no adverse events? Only one thing can follow: when the medicine kills, someone else must be blamed. This is not a hypothetical. It is a mechanical prediction. If the drug cannot fail, the patient must have failed — or the patient’s caretaker. The public-health machine has known this for at least three generations, and it has structured its institutions accordingly:
- When a vaccinated infant dies in the crib, the death becomes “SIDS” — a diagnostic category that literally means we do not know what killed the child, but we assure the parents it was not the shots.[15][32]
- When SIDS statistics become embarrassing, the deaths are reclassified as “accidental suffocation in bed,” and the parents are counseled about safe-sleep practices they did not violate.[33]
- When “accidental suffocation” cannot explain a case — because, for example, both twins died in the same night in the same crib, a statistical near-impossibility — the death is escalated to homicide. The parent is arrested. The vaccine record is sealed as “irrelevant” to the criminal proceeding. The autopsy is withheld from the public until after the criminal trial. The pediatrician who administered five simultaneous injections over the parents’ warning is never questioned. The manufacturer whose adjuvants and antigens circulated through the infant brainstem is never named in the indictment. The ER physician who documented the “post-immunization reaction” is not called as a witness against the vaccine — only, if at all, against the mother.
This is what every parent of a vaccine-injured child has understood for decades. When Barbara Loe Fisher and Harris Coulter published DPT: A Shot in the Dark in 1985 — documenting infant deaths within forty-eight hours of DPT vaccination — the response of the pediatric establishment was not to investigate the deaths but to accuse Fisher of endangering public health. When William Parker published evidence that acetaminophen-vaccine interaction was a probable trigger of regressive autism, his Duke laboratory was closed on the recommendation of a department chaired by administrators who sat on Johnson & Johnson’s board.[35] When investigators raise safety concerns about combination pediatric vaccines, their careers are systematically ended in a manner unprecedented in modern medical history. The message to every subsequent investigator has been unmistakable: publish the wrong finding and your career ends. Report the wrong death and your child was smothered.
Andrea Shaw is not an isolated case. She is the predictable output of a public-health information architecture that requires — as a matter of institutional survival — that vaccine deaths not exist. Because if they exist, the entire edifice of universal childhood vaccination as a moral imperative collapses into what it actually is: a risk-benefit calculation that must be made, honestly and case by case, by informed parents and their physicians, with full disclosure of susceptibility factors, lot data, and combination-exposure risks. The blanket safety claim exists to prevent that calculation from happening. And the cost of preventing that calculation, for the past fifty years, has been paid by the children who die and, increasingly, by the parents who are then charged with their murder.
The machinery that produced Andrea Shaw’s indictment did not begin in Payette, Idaho, in July 2026. It began in 1979, when the ICD code was eliminated. It continued in 1986, when manufacturer liability was stripped. It hardened in the 1990s, when “Back to Sleep” reclassification laundered the SIDS numbers. It calcified in the 2000s, when CDC and AAP messaging converged on the phrase “safe and effective” as an incantation to be repeated without qualification. It reached its logical terminus the moment a prosecutor in Idaho looked at a case of simultaneous twin death within a week of five vaccinations plus emergency-room acetaminophen and concluded that the only reasonable explanation was that the mother did it.
The victims of this system are not only the dead children. They are also their parents. And they will continue to be their parents — criminalized, incarcerated, driven to suicide, separated from their surviving children — until the public-health establishment is forced to acknowledge what its own literature has documented for eighty years: that vaccines, like every other pharmaceutical, can and do kill some children some of the time, and that the pretense otherwise is not science but sacrament.
What Justice Would Look Like
The evidence base assembled above is not new. Substantially all of it was available in 2007. Most of it was available in 1985. The Werne and Garrow case has been in the literature for eighty years. What is new is that we now have two additional lines of evidence that were not available even in 2015: (a) the direct biochemical documentation of NAPQI generation and glutathione depletion as the acetaminophen mechanism of neurotoxicity (Parker et al. 2024[26]), and (b) the Boston Birth Cohort’s cord-blood biomarker confirmation of the acetaminophen-autism dose-response.[30] The synergy between these two exposures is no longer speculative. It is the most parsimonious explanation of the pattern.
The state of Idaho is prosecuting Andrea Shaw for homicide on the theory that she smothered both of her toddlers in the same night, in the same bed, without a witness, without a motive, without any forensic evidence beyond a nonspecific finding of pulmonary vascular congestion that is entirely consistent with the alternative etiology. It is doing so at the same time that:
- Health and Human Services Secretary Robert F. Kennedy Jr. is preparing to formally acknowledge the acetaminophen-autism link,[38]
- The National Vaccine Injury Compensation Program continues to pay families whose vaccinated children died of “SIDS,”[34]
- The IOM has already conceded that vaccines can cause fatal anaphylaxis in infants on the basis of the identical fact pattern in the Werne and Garrow case,[14]
- And the peer-reviewed medical literature contains at least eight prior sets of twins who died together after vaccination, none of whose mothers were charged with murder.[25]
Justice would require, at minimum:
- Immediate exhumation-quality re-examination of the Shaw twins’ brainstems and cardiac conduction systems under the Ottaviani protocol, by a pathologist with expertise in vaccine-associated infant death rather than routine forensic pathology.
- Formal quantitation of NAPQI-protein adducts in hepatic and cerebral tissue, and of beta-tryptase in serum, to evaluate the acetaminophen contribution to the terminal event.
- Full disclosure of the vaccine lot numbers administered on April 23, 2025, with cross-referencing against VAERS reports for those lots — the FDA has known since 1979 that “hot lots” cluster infant deaths, and confidential manufacturer memos have historically instructed distributors to disperse suspect lots geographically to avoid detectable clusters.[39]
- Dismissal of the murder indictment and re-classification of the deaths as vaccine-associated sudden death pending independent forensic review.
Whether Andrea Shaw ever holds her surviving newborn outside of a prison visiting room depends on whether her defense team is permitted to introduce this evidence, and whether the presiding judge is willing to consider that a pattern documented in the peer-reviewed medical literature since 1946 might be more parsimonious than the alternative theory that a twenty-three-year-old mother suffocated both of her children on the same night without leaving forensic traces.
The Shaw twins did not die from smothering. They died from a poisoning that our medical infrastructure is institutionally incapable of naming. Their mother did not kill them. A regulatory-industrial complex that will not permit its products to fail killed them, and is now preparing to have their mother killed — or caged for life — for the crime of trusting it. This is what happens, always and inevitably, when a government-pharmaceutical alliance declares that its interventions are universally safe: the victims of those interventions become the criminals. It has happened to Andrea Shaw. It will happen to the next mother, and the next, until enough of us refuse the slogan and demand the science.
Until we are willing to name what killed Dallas and Tyson Shaw, we will continue to bury the children and prosecute the parents.

Author’s note
This piece is one in a series examining the intersection of pediatric vaccination policy, acetaminophen exposure, and infant mortality. A prior installment (“Broken Trust: The Tylenol Cover-Up That May Have Damaged Millions of Children”) documented the William Parker–Duke University–Johnson & Johnson conflict-of-interest architecture. A forthcoming installment will address the Ottaviani neuropathological protocol and the international pharmacovigilance signal for hexavalent vaccines in detail. A subsequent installment will address the Andrea Shaw defense strategy.
If you are a pediatrician, forensic pathologist, or medical examiner with knowledge or documentation relevant to the Shaw case, please contact the author through Children’s Health Defense or through the comments below.
Notes and citations
[^1]: Sara Regensberg, “The Shaw Twins Didn’t Die From SIDS,” Substack, 2025, https://open.substack.com/pub/sararegensberg/p/the-shaw-twins-didnt-die-from-sids; Isabelle Taft, “Plaintiff for Anti-Vaccine Group’s Suit Is Charged With Murder of Her Twins,” New York Times, July 7, 2026, https://www.nytimes.com/2026/07/07/us/idaho-twins-death-shaw-vaccines-murder.html.
[^2]: Pierre Kory, “Medical Record Review of the Twins Who Died After Vaccination and a Review of the Literature Proving SIDS Is Caused by Vaccines,” Pierre Kory’s Medical Musings, June 23, 2025, https://pierrekorymedicalmusings.com/p/medical-record-review-of-the-twins.
[^3]: Zachary Stieber, “Experts Ruled Out Vaccines in Deaths of Twins, Prosecutors Say,” The Epoch Times, July 15, 2026, https://www.theepochtimes.com/us/experts-ruled-out-vaccines-in-deaths-of-twins-prosecutors-say-6062060.
[^4]: American Academy of Pediatrics, Red Book: Report of the Committee on Infectious Diseases, 32nd ed. (Itasca, IL: AAP, 2021), routine recommendation for acetaminophen management of post-vaccination fever.
[^5]: Michael Duke, “Objection to Motion to Reduce Bond, State of Idaho v. Andrea Renee Shaw,” Payette County District Court, July 13, 2026, cited in The Epoch Times, July 15, 2026.
[^6]: Michael H. Malloy and Howard Freeman, “Sudden Infant Death Syndrome Among Twins,” Archives of Pediatrics and Adolescent Medicine 153, no. 7 (July 1999): 736–740, https://pubmed.ncbi.nlm.nih.gov/10401808/.
[^7]: Millard Bass, cited in Neil Z. Miller, “Vaccines and Sudden Infant Death: An Analysis of the VAERS Database 1990–2019 and Review of the Medical Literature,” Toxicology Reports 8 (2021): 1324–1335, https://pmc.ncbi.nlm.nih.gov/articles/PMC8255173/.
[^8]: J. Werne and I. Garrow, “Fatal Anaphylactic Shock: Occurrence in Identical Twins Following Second Injection of Diphtheria Toxoid and Pertussis Antigen,” Journal of the American Medical Association 131, no. 9 (1946): 730–735.
[^9]: S. C. Roberts, “Vaccination and Cot Deaths in Perspective,” Archives of Disease in Childhood 62, no. 7 (1987): 754–759, https://pmc.ncbi.nlm.nih.gov/articles/PMC1779219/.
[^10]: Harris L. Coulter and Barbara Loe Fisher, DPT: A Shot in the Dark (New York: Harcourt Brace Jovanovich, 1985), 88–92.
[^11]: Yasemin Balci et al., “Simultaneous Sudden Infant Death Syndrome,” Journal of Forensic and Legal Medicine 14, no. 2 (February 2007): 87–91, https://www.sciencedirect.com/science/article/abs/pii/S1353113106000071.
[^12]: E. A. Mitchell et al., “Simultaneous Sudden Unexpected Death in Infancy of Twins: Case Report,” International Journal of Legal Medicine 125, no. 1 (January 2011): 143–146, https://pubmed.ncbi.nlm.nih.gov/20082088/.
[^13]: Huang et al., cited in Neil Z. Miller and Brian S. Hooker, “Vaccines and Sudden Infant Death: An Analysis of the VAERS Database 1990–2019 and Review of the Medical Literature,” Toxicology Reports 8 (2021): 1324–1335.
[^14]: Institute of Medicine, Immunization Safety Review: Vaccinations and Sudden Unexpected Death in Infancy (Washington, DC: National Academies Press, 2003), https://www.ncbi.nlm.nih.gov/books/NBK221473/.
[^15]: Hannah C. Kinney and Bradley T. Thach, “The Sudden Infant Death Syndrome,” New England Journal of Medicine 361, no. 8 (August 20, 2009): 795–805.
[^16]: A. Vege and T. O. Rognum, “Inflammatory Responses in Sudden Infant Death Syndrome — Past and Present Views,” FEMS Immunology and Medical Microbiology 25, no. 1–2 (1999): 67–78.
[^17]: Giulia Ottaviani, Anna Maria Lavezzi, and Luigi Matturri, “Sudden Infant Death Syndrome (SIDS) Shortly After Hexavalent Vaccination: Another Pathology in Suspected SIDS?” Virchows Archiv 448, no. 1 (January 2006): 100–104, https://pubmed.ncbi.nlm.nih.gov/16231176/.
[^18]: Anna Maria Lavezzi et al., “Sudden Infant Death Following Hexavalent Vaccination: A Neuropathologic Study,” Current Medicinal Chemistry 21, no. 32 (2014): 3697–3705, https://pubmed.ncbi.nlm.nih.gov/24083600/.
[^19]: B. Zinka et al., “Unexplained Cases of Sudden Infant Death Shortly After Hexavalent Vaccination,” Vaccine 24, no. 31–32 (July 26, 2006): 5779–5780, https://pubmed.ncbi.nlm.nih.gov/15908063/.
[^20]: R. von Kries et al., “Sudden and Unexpected Deaths After the Administration of Hexavalent Vaccines (Diphtheria, Tetanus, Pertussis, Poliomyelitis, Hepatitis B, Haemophilus influenzae Type B): Is There a Signal?” European Journal of Pediatrics 164, no. 2 (February 2005): 61–69, https://pubmed.ncbi.nlm.nih.gov/15602672/.
[^21]: Giuseppe Traversa et al., “Sudden Unexpected Deaths and Vaccinations During the First Two Years of Life in Italy: A Case Series Study,” PLoS ONE 6, no. 1 (January 26, 2011): e16363, https://pmc.ncbi.nlm.nih.gov/articles/PMC3027668/.
[^22]: Ronny Kuhnert et al., “Reanalyses of Case-Control Studies Examining the Temporal Association Between Sudden Infant Death Syndrome and Vaccination,” Vaccine 30, no. 13 (March 16, 2012): 2349–2356.
[^23]: Neil Z. Miller and Gary S. Goldman, “Infant Mortality Rates Regressed Against Number of Vaccine Doses Routinely Given: Is There a Biochemical or Synergistic Toxicity?” Human and Experimental Toxicology 30, no. 9 (September 2011): 1420–1428, https://journals.sagepub.com/doi/10.1177/0960327111407644.
[^24]: Gary S. Goldman and Neil Z. Miller, “Relative Trends in Hospitalizations and Mortality Among Infants by the Number of Vaccine Doses and Age, Based on the Vaccine Adverse Event Reporting System (VAERS), 1990–2010,” Human and Experimental Toxicology 31, no. 10 (October 2012): 1012–1021, https://journals.sagepub.com/doi/10.1177/0960327112440111.
[^25]: Neil Z. Miller and Brian S. Hooker, “Vaccines and Sudden Infant Death: An Analysis of the VAERS Database 1990–2019 and Review of the Medical Literature,” Toxicology Reports 8 (2021): 1324–1335, https://pmc.ncbi.nlm.nih.gov/articles/PMC8255173/.
[^26]: William Parker et al., “The Dangers of Acetaminophen for Neurodevelopment Outweigh Scant Evidence for Long-Term Benefits,” Children 11, no. 1 (2024): 44, https://www.mdpi.com/2227-9067/11/1/44.
[^27]: Rosemary H. Waring and L. V. Klovrza, “Sulphur Metabolism in Autism,” Journal of Nutritional and Environmental Medicine 10, no. 1 (2000): 25–32.
[^28]: John P. Jones III et al., “Evaluating the Role of Susceptibility Inducing Cofactors and of Acetaminophen in the Etiology of Autism Spectrum Disorder,” Life 14, no. 8 (2024): 918.
[^29]: Stephen T. Schultz et al., “Acetaminophen (Paracetamol) Use, Measles-Mumps-Rubella Vaccination, and Autistic Disorder: The Results of a Parent Survey,” Autism 12, no. 3 (May 2008): 293–307.
[^30]: Yuelong Ji et al., “Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure With Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood,” JAMA Psychiatry 77, no. 2 (February 2020): 180–189.
[^31]: Ann Z. Bauer et al., “Paracetamol Use During Pregnancy — A Call for Precautionary Action,” Nature Reviews Endocrinology 17, no. 12 (December 2021): 757–766.
[^32]: Sayer Ji, “131 Ways for an Infant to Die: How SIDS Camouflages Vaccine Injury,” GreenMedInfo, https://greenmedinfo.com/blog/131-ways-infant-die.
[^33]: Michael H. Malloy and Marian F. MacDorman, “Changes in the Classification of Sudden Unexpected Infant Deaths: United States, 1992–2001,” Pediatrics 115, no. 5 (May 2005): 1247–1253.
[^34]: U.S. Health Resources and Services Administration, National Vaccine Injury Compensation Program, monthly statistics reports, https://www.hrsa.gov/vaccine-compensation.
[^35]: Jennifer Margulis, “Top Professor Ousted as His Research on Tylenol Became Too Much of a Headache for His University and Big Pharma,” The Epoch Times, 2023.
[^36]: Sayer Ji, “Epidemic of Sudden Infant Deaths a Medically-Induced Syndrome,” GreenMedInfo, https://greenmedinfo.com/blog/epidemic-sudden-infant-deaths-medically-induced-syndrome-1, citing beta-tryptase elevation in a 2008 Forensic Science International case report.
[^37]: Cited in Sayer Ji, “131 Ways for an Infant to Die”; source data: Japanese Ministry of Health, Labour and Welfare compensation statistics 1970–1990.
[^38]: “RFK Jr., HHS to Link Autism to Tylenol Use in Pregnancy and Folate Deficiencies,” Wall Street Journal, September 2025, reported by Kenvue interim CEO lobbying meetings, September 2025.
[^39]: See discussion of Tennessee 1978 DPT lot-clustering incident in “Please Help Prevent a Medical Miscarriage of Justice,” The Midwestern Doctor, https://www.midwesterndoctor.com/p/please-help-prevent-a-medical-miscarriage.
[^40]: William Parker, personal communication regarding manuscript rejections on procedural rather than scientific grounds, cited in Jennifer Margulis, “Top Professor Ousted as His Research on Tylenol Became Too Much of a Headache for His University and Big Pharma,” The Epoch Times, 2023, https://www.theepochtimes.com.
[^40a]: Lisa P., “What a Landmark Case in Britain Could Mean for Mother Charged in Idaho Twins’ Deaths,” The Defender (Children’s Health Defense), July 15, 2026, https://childrenshealthdefense.org/defender/angela-cannings-england-landmark-case-meaning-idaho-mother-charged-twins-deaths/. The Court of Appeal decision is R v Cannings EWCA Crim 01. See also R v Clark EWCA Crim 1020.
© 2026. This work is licensed for full or partial republication for educational, journalistic, and legal purposes. Please cite as: Ji, Sayer. “The Shaw Twins Didn’t Suffocate. They Were Poisoned Twice.” Substack, July 2026.
____
https://sayerji.substack.com/p/the-shaw-twins-didnt-suffocate-they?