
By Nicolas Hulscher, Dr. Charles Hoffe, and Prof Michel Chossudovsky
Global Research

Introductory Note
We bring to the attention of our readers this outstanding article by Dr. Nicolas Hulscher pertaining to the amyloid microclots circulating in the blood vessels of Covid vaccinated people.
I should mention that Dr. Charles Hoffe came to similar conclusions at the outset of the Covid Vaccine in early 2021.
Dr. Charles Hoffe referred to Microscopic Blood Clots as Hidden Covid-19 Vaccine Injuries,
Many people who are vaccinated will not be immediately aware of the injuries incurred.
The latter in many cases of “adverse events” are not discernible nor are they recorded. While “big blood clots” resulting from the vaccine are revealed and reported by those vaccinated, an important study by Canada’s Dr. Charles Hoffe suggests that the mRNA vaccine generates “microscopic blood clots”.
“The blood clots we hear about which the media claim are very rare are the big blood clots which are the ones that cause strokes and show up on CT scans, MRI, etc.
The clots I’m talking about are microscopic and too small to find on any scan. They can thus only be detected using the D-dimer test.”
“These people have no idea they are even having these microscopic blood clots.
The most alarming part of this is that there are some parts of the body like the brain, spinal cord, heart and lungs which cannot re-generate. When those tissues are damaged by blood clots they are permanently damaged.
“These shots are causing huge damage and the worst is yet to come.” (Charles Hoffe, see p. 108-109)
Michel Chossudovsky, Global Research, November 18, 2025
*****
Video Charles Hoffe. Microscopic Blood Clots
Watch below his interview with Laura Lynn Tylor Thompson (also available on Rumble channel).
Video: “Biggest Disaster in Medical History”. Dr. Charles Hoffe
****
Anomalous Amyloid Microclots Found in 100% of the COVID-19 Vaccinated
by Nicolas Hulscher
November 18, 2025
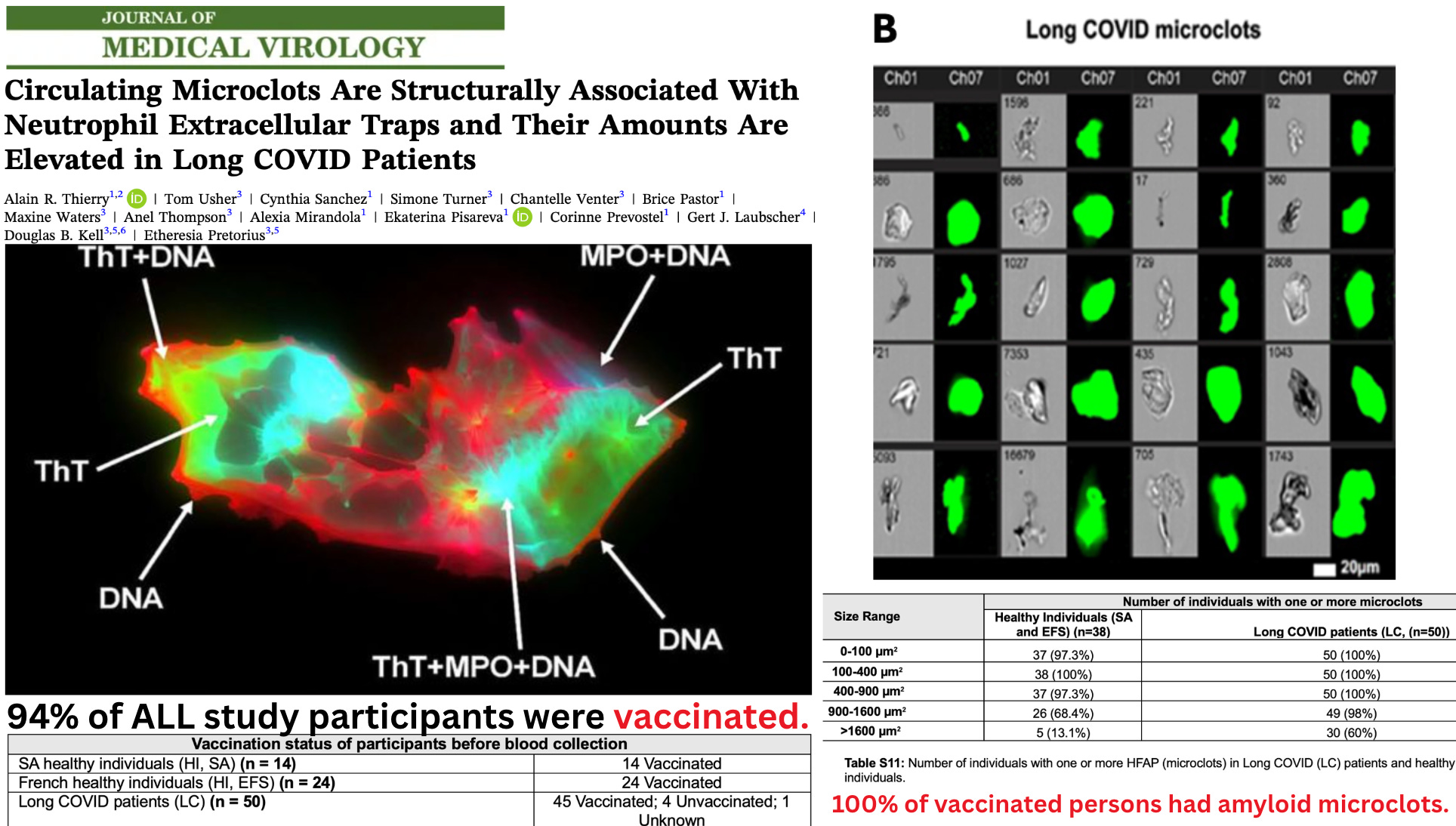
A new peer-reviewed study has quietly revealed one of the most consequential biological findings of the pandemic era — and the authors never acknowledge it:
Every single vaccinated participant in the study had fibrinolysis-resistant, ThT-positive amyloid microclots circulating in their blood.
Hidden in the supplementary tables is a demographic and biochemical pattern that completely reframes the paper:
94% of all participants were vaccinated. 100% of these vaccinated individuals had amyloid microclots — including every “healthy control.”
The condition labeled “Long COVID” occurred almost entirely in a heavily vaccinated population, without any laboratory confirmation of prior SARS-CoV-2 infection. In reality, the study is observing Long VACCINE pathology, not Long COVID.
And because the authors’ own mechanistic experiments show that purified spike protein alone produces these amyloid, fibrinolysis-resistant clots, the implications are profound.
All individuals in the study — 100% of the vaccinated — had amyloid microclots.
Researchers identified microclots using Thioflavin-T (ThT), an amyloid-binding fluorogenic dye. ThT positivity was the defining criterion. A structure was only counted as a microclot if it bound ThT.
Therefore, every microclot counted in the study is, by definition, amyloidogenic.
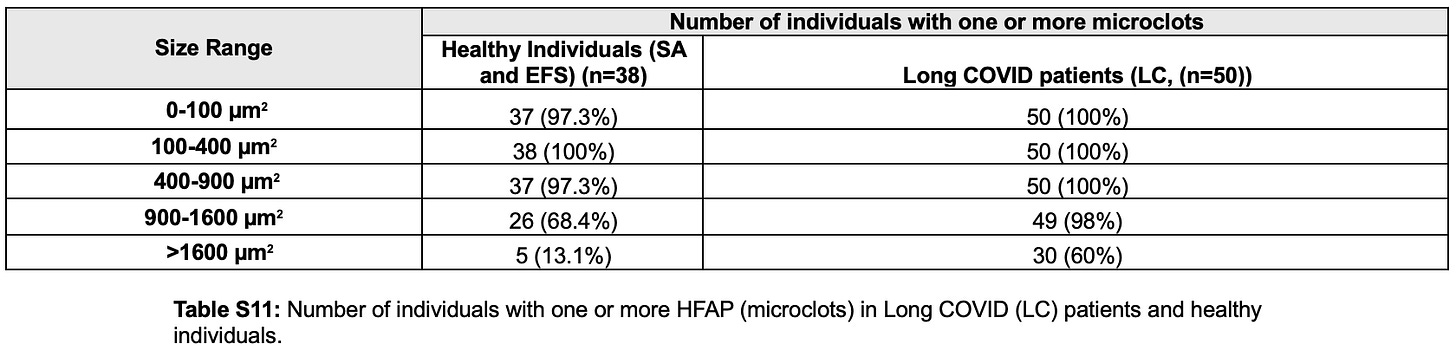
And according to Table S11, every single vaccinated participant had amyloid microclots in multiple size ranges:
Because 83 of 88 participants (94%) were vaccinated, this means:
Every vaccinated person in the study had amyloid microclots.
“Long COVID” (Long VACCINE) patients had extreme elevations in large, pathological amyloid microclots.
Small amyloid microclots were present in everyone, but the pathological burden differed sharply.
According to Table S11:
- 98% of “Long COVID” (Long VACCINE) patients had large microclots in the 900–1600 µm² range
- 60% had very large microclots >1600 µm²
- Total microclot burden was ~20-fold higher in “Long COVID” patients
These larger, pathogenic amyloid microclots were densely packed with:
- Neutrophil extracellular traps (NETs)
- Myeloperoxidase
- Neutrophil elastase
- Extracellular DNA
- Misfolded amyloid fibrin
COVID-19 Infection Was Never Verified
Despite positioning the results as a hallmark of “Long COVID,” none of the participants were confirmed to have had SARS-CoV-2 infection. The study performed:
- no antibody testing
- no PCR
- no sequencing
- no neutralizing antibody assays
Long COVID status was assigned purely via symptoms and clinician impression. There is no evidence in the study that any participant was biologically positive for prior infection.
Thus, the clotting abnormalities cannot be attributed specifically to infection, but rather to vaccination.
Spike Protein Alone Produced Identical Amyloid Microclots
In a mechanistic experiment, the authors added purified spike protein to fibrinogen.
This single intervention produced:
- insoluble, ThT-positive amyloid microclots
- misfolded fibrin structures identical to those in patient samples
- fibrinolysis-resistant aggregates compatible with vessel obstruction
The authors confirmed that Spike protein directly induces amyloid microclot formation, corroborating previous studies.
Explains Prevalent White Fibrous Clots Found in the Dead
The study’s core findings — 100% amyloid microclots in vaccinated individuals and direct spike-induced amyloid fibrin formation — offer a clear mechanism for the large, rubbery white fibrous clots increasingly reported in deceased individuals since 2021.
At the 2025 Tennessee Funeral Directors Association (TFDA) convention, former USAF Major Tom Haviland conducted the first state-level survey of embalmers:
- 64% reported white fibrous clots in 2025
- Found in 17% of all bodies
- 70% observed widespread microclotting (“coffee-grounds blood”)
- 39% reported rising infant deaths (+14%)
Forensic analysis by Kevin W. McCairn, PhD et al shows that these postmortem clots:
- are amyloidogenic fibrin aggregates, not normal thrombi
- exhibit β-sheet structures (ThT-positive)
- are protease-resistant, rubbery, and fibrous
- have dense fibrillar ultrastructure on SEM
- contain human genetic material
- and show preliminary plasmid/spike-associated markers

These characteristics match exactly the pathological microclots described in the new study — only at a later, aggregated, end-stage form.
The progression is biologically straightforward:
- Spike exposure (infection or mRNA vaccination)
- Amyloid microclots form — present in 100% of vaccinated subjects
- Large, NET-rich, fibrinolysis-resistant clots accumulate (20× higher in Long vaccine patients)
- These merge into massive, rubbery, white fibrous intravascular clots
This new study documents the early and intermediate stages in the living; Haviland’s surveys and McCairn’s analysis reveals the final stage in the dead.
Conclusions
Although the authors frame their findings as “Long COVID,” the underlying data reveal something far more consequential:
- 100% of vaccinated participants had amyloid microclots.
- Large, fibrinolysis-resistant amyloid microclots were concentrated in the Long vaccine group.
- No participant had laboratory-confirmed SARS-CoV-2 infection.
- Spike protein alone produced identical amyloid microclots in vitro.
- With 94% vaccination uptake, the biological signal is overwhelmingly linked to spike exposure in a vaccinated population.
These findings carry serious public-health implications:
- Every vaccinated individual in the study showed early-stage amyloid microclots, raising alarms about cumulative vascular injury across the entire globe.
- The pathology mirrors the large white fibrous clots now documented by embalmers and forensic analysts.
And critically:
- The CDC and federal public-health agencies must finally do their job and launch an immediate, transparent investigation into these findings.
- Failing to intestigate the white fibrous clot situation constitutes a dereliction of duty.
- Any platform delivering spike protein into human circulation must be immediately banned for human use.
Nicolas Hulscher, MPH, Epidemiologist and Foundation Administrator, McCullough Foundation
Featured image source